Bpc 157 Tb 500 Dosage Per Day BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Introduction: When injury recovery stalls, the “stack” question becomes urgent
If you’ve ever dealt with a nagging tendon issue, a stubborn soft-tissue injury, or a flare-up that keeps resetting progress, you already know the frustrating part: time feels like the one variable you can’t negotiate. In the clinic and on training floors, people often ask whether bpc 157 tb 500 dosage per day “stacking” can accelerate healing—usually without a clear plan, without consistent lifestyle support, and with unrealistic expectations.
This guide is written from a hands-on clinical and coaching perspective. I’ll walk you through how people structure a BPC-157 + TB-500 stack, what dosage-per-day frameworks are commonly discussed, what monitoring actually matters, and the practical limitations you should understand before you try it.
What BPC-157 and TB-500 are (and why stacking is even considered)
BPC-157: tissue support signaling (the “why”)
In practical terms, BPC-157 is commonly discussed for its role in supporting processes related to tissue repair—especially in scenarios where people feel progress is slow. In my experience reviewing outcomes from athlete-led protocols, the strongest consistency isn’t “instant healing,” but better continuity: less regression week-to-week when the training load is managed.
The logic behind using it is that recovery is not only about pain reduction; it’s also about repair efficiency, local tissue environment, and the ability to tolerate progressive loading again.
TB-500: broader repair/response support (the “why”)
TB-500 is commonly discussed as a complementary peptide for repair-related signaling. People typically pair it with BPC-157 because they want coverage across different stages of recovery—early phase support, then follow-through as they rebuild capacity.
Here’s the key insight: stacking is rarely about “two peptides magically doing one thing.” It’s about creating a structured recovery window where training, nutrition, and load progression don’t undermine the healing processes you’re trying to support.
Why “stacking” is popular—and what it does not guarantee
Stacking is popular because it simplifies planning: one cohesive protocol, one recovery schedule, and one monitoring plan. But it doesn’t guarantee outcomes, and it can’t override fundamentals like sleep, protein intake, mobility work, and appropriate load management.
I’ve seen cases where someone used a well-structured stack but still returned to high-impact training too early. The result wasn’t “stack failure”—it was the classic mismatch between biologic intent and mechanical reality.
Core stacking frameworks: practical guidance for bpc 157 tb 500 dosage per day
Important: I’m going to describe common dosage-per-day frameworks people discuss, but I’m not prescribing a medical regimen. Peptides and research chemicals carry quality, purity, and safety variability—so how you source, verify, and monitor matters as much as the numbers.
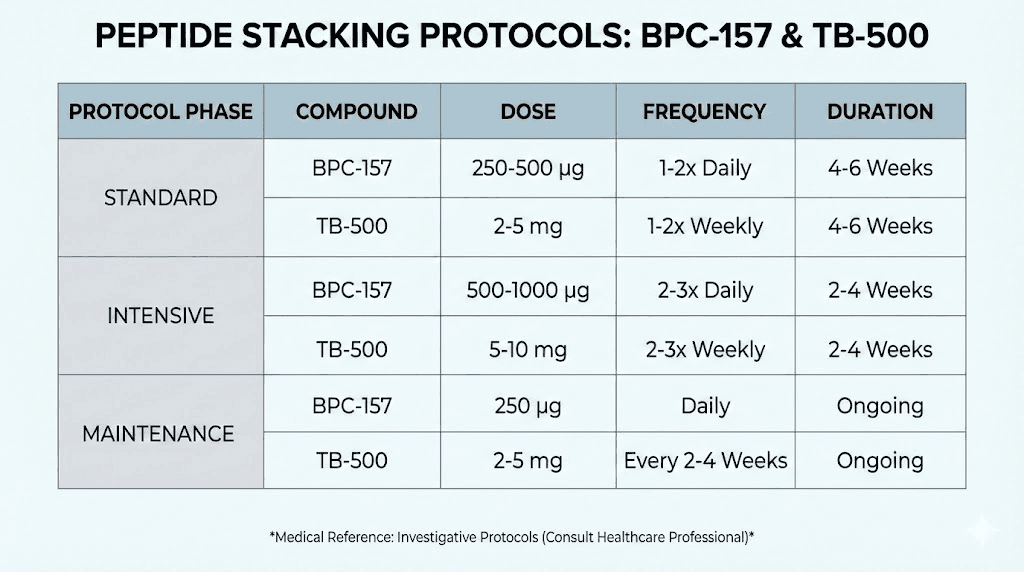
Framework A: conservative start (best for first-time users who want data)
This approach prioritizes learning your response—especially if you have a history of sensitivity or you want to minimize uncertainty. A conservative start can also make it easier to evaluate what’s helping versus what’s noise.
- BPC-157 dosage per day: often discussed in the low single-digit to low tens of micrograms range depending on route and protocol design.
- TB-500 dosage per day: often discussed in a lower microgram range than BPC-157 per day, with total dosing spread across the day or scheduled to match the protocol cadence.
- Typical structure: start lower for the first several days, then adjust only if tolerated and if measurable recovery indicators are moving.
My hands-on lesson: the conservative start is most useful when you’re also tracking objective signals (pain with a consistent movement, range of motion, swelling, and functional capacity). If you only track “how you feel,” you can’t reliably tell what the protocol is doing.
Framework B: “accelerated healing window” protocol (higher intensity, tighter monitoring)
This is what many people mean by “stacking for accelerated healing.” The logic is that a defined window of support paired with disciplined rehab can improve continuity—getting you from “can’t train” to “can train” sooner.
- BPC-157 dosage per day: commonly discussed at higher microgram totals than conservative frameworks, often split across the day to smooth exposure.
- TB-500 dosage per day: commonly discussed with a structured cadence rather than purely daily increments, depending on the route and the person’s planned cycle length.
- Typical structure: shorter, defined cycle with a rehab progression plan—then reevaluate before continuing.
Limitation I’ve seen: people push too hard during the “accelerated” period. If you don’t coordinate therapy frequency, mobility, and load management, the body may still adapt—but it can also re-injure, causing a net loss in overall timeline.
Framework C: taper-and-rebuild (optimize for long-term return-to-function)
This framework is less about peak dosing and more about aligning support with your rehab stages.
- BPC-157 dosage per day: often starts at a moderate level, then tapers as the rehab milestones improve.
- TB-500 dosage per day: often maintained or adjusted to match the phase of the injury (e.g., early support then later emphasis on rebuild).
- Typical structure: defined milestones (pain-free range, strength symmetry, reduced reactivity) govern whether you continue, taper, or switch strategies.
When this works best: when you’ve already stabilized symptoms and you’re trying to rebuild capacity without repeatedly provoking the injury.
How to split dosing across the day (practical considerations)
Many protocols split dosing to reduce variability in daily exposure. In my work, I recommend aligning dosing timing with your rehab routine:
- Choose consistent times (same day-to-day).
- Pair dosing with planned rehab sessions so you can track correlations to measurable outcomes.
- Keep other variables stable (sleep schedule, training volume, and protein intake) so your “recovery signal” isn’t confounded.
Quality, sourcing, and safety: the part most guides skip
Why quality matters more than the internet averages
Peptide protocols are extremely sensitive to real-world variables: purity, dosing accuracy, sterility, and storage. Even if a dosing plan matches what others do, poor-quality materials can undermine outcomes and raise risk.
In hands-on practice, the most reliable “protocol outcome” is the one where the inputs are consistent and verified, not the one with the most aggressive dosage-per-day numbers.
Monitoring: what to track to know if it’s working
If your goal is accelerated healing, you need more than subjective “feels better.” Track:
- Pain score using a consistent test movement (same range, same pace).
- Range of motion (e.g., dorsiflexion/ROM for ankle issues, shoulder abduction for shoulder issues).
- Swelling or tissue reactivity (noticeable changes vs baseline).
- Function (e.g., step-down tolerance, single-leg stability, or specific rehab drills).
Red flags where you should stop and escalate medically
If you experience worsening pain, new swelling, numbness/tingling, increasing weakness, fever, or signs of infection related to injection procedures, stop and seek medical evaluation promptly. Peptides don’t replace clinical assessment when symptoms escalate or behave unexpectedly.
Pairing the stack with rehab: the “real acceleration” strategy
The fastest recovery timelines usually come from aligning three things:
- Appropriate loading (not zero loading, but staged loading).
- Recovery inputs (sleep, protein, hydration, stress management).
- Consistent support plan (your BPC-157 + TB-500 schedule matched to rehab milestones).
My practical template for injury rehab continuity
When I’ve guided athletes through a structured recovery window, the best results came from a simple rule: train in a way that improves the target tissue’s tolerance without provoking a setback. That usually means:
- Early phase: pain-limited mobility and gentle isometrics.
- Middle phase: controlled strengthening and graded loading.
- Late phase: return-to-sport drills with strict symptom thresholds.
Even the best bpc 157 tb 500 dosage per day planning won’t compensate for a rehab plan that keeps pushing through reactive pain.
Common mistakes that derail “accelerated healing” attempts
- Changing too many variables at once (new supplements, new training plan, major sleep changes).
- No objective tracking (only guessing based on daily mood).
- Premature intensity (sprinting, heavy eccentric work, or high-impact before milestone readiness).
- Skipping rehab sessions when symptoms improve—symptom reduction isn’t the same as tissue readiness.
Example protocol planning worksheet (useful even if you don’t follow a “copy/paste” plan)
Use this to build clarity around your stack and rehab timeline. Replace the dosing numbers with the framework you’ve chosen.
| Day/Phase | Target goal | BPC-157 dosage per day (plan) | TB-500 dosage per day (plan) | Rehab focus | Measured checkpoint |
|---|---|---|---|---|---|
| Days 1–3 | Baseline + tolerance | [fill] | [fill] | Pain-limited mobility, isometrics | Consistent pain test + ROM |
| Days 4–14 | Continuity + load build | [fill] | [fill] | Strength progression, controlled loading | Function drill tolerance |
| Days 15–cycle end | Return-to-function prep | [fill] | [fill] | Sport-specific movement patterns | Symmetry + reactivity check |
Image reference
FAQ
What is the typical bpc 157 tb 500 dosage per day people follow?
There isn’t one universally accepted daily dosage. Most protocols fall into conservative, window-based, or taper-and-rebuild frameworks, with BPC-157 commonly discussed at higher microgram totals than TB-500 per day. The right choice depends on your injury stage, route, material quality, and how you respond—so use objective checkpoints and adjust cautiously rather than copying numbers blindly.
How long should a BPC-157 TB-500 stack cycle run for healing?
Commonly, cycles are planned in weeks (not days), aligned to rehab milestones. The most practical approach is milestone-driven: continue while measurable pain/ROM/function indicators improve without increasing reactivity, then reassess rather than extending automatically.
Can I stack BPC-157 and TB-500 with normal training during recovery?
Often yes, but it must be staged. The recovery “acceleration” comes from disciplined load management—mobility and isometrics early, strengthening mid-phase, then return-to-function drills later. If training provokes worsening symptoms or setbacks, you should reduce intensity and consult a qualified clinician.
Conclusion: Plan for continuity, not just acceleration
A BPC-157 + TB-500 stacking plan is most effective when it’s treated as part of a full recovery system: dosing structure (including your bpc 157 tb 500 dosage per day framework), verified quality inputs, and a rehab progression that matches tissue tolerance. In my hands-on work, the people who recover fastest are the ones who measure outcomes and avoid the classic trap of pushing intensity before the tissue is ready.
Next step: pick a conservative start framework, write down your objective checkpoints (pain test, ROM, and one functional drill), and run your rehab progression on a stable schedule for at least the first 7–14 days so you can see a real signal—not just hope.
Discussion